Fat Grafting: Body

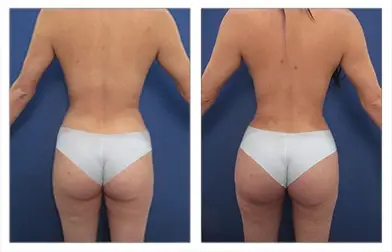
FAT GRAFTING BODY BEFORE AND AFTER







Understanding Fat Grafting Body
Fat grafting body has become a mainstay of the plastic surgeon’s armamentarium and allows previously untreatable deformities to be corrected and body contouring outcomes to be optimized.
Patients benefiting from Los Angeles fat transfer techniques include:
- patients who have developed breast deformities following failed implant augmentation.
- breast reconstruction patients who require improvement of breast mound contour irregularities.
- patients who have observed disproptiontely smaller buttock cheek volumes
- primary buttock augmentation patients with poor results.
Both groups of fat grafting body patients benefit from the ability of fat cells to be used, much like putty, to not only augment the entire breast mound but also to correct minor breast mound contour irregularities as well as to augment their buttocks and correct minor butt cheek contour irregularities.
Lost Angeles Cosmetic Surgeon specialist at SurgiSculpt will examine your breast and buttock contour and take detailed notes and measurements to ensure optimal fat grafting body results.
- First, liposuction is used to harvest and collect fat material using sterile conditions.
- Next, the fat material is processed to remove an oily and liquid layer and to prepare for transfer back to your body. Desired volumes for the fat grafting body are dependent on the transfer site. While revision cases will typically require less than 100cc of fat transfer, primary cases may require as much as 1000cc of fat transfer.
- Fat cells are transferred back to the breast and buttock by feathering the cells into the desired areas needing volume replacement.
A critical principle of the fat grafting body revolves around maximizing the grafted fat cell surface area to volume ratio in an attempt to re-establish blood supply to the transplanted and ischemic cells. Two maneuvers are used to ensure optimum graft take and they include the transfer of fat grafts in individual 0.5cc to 1.0cc fat packs as well as layering the fat packs in multiple planes including above the muscle, fascia, deep and superficial fat. The wide distribution of fat cells in small packs optimizes graft take and subsequent results.
Breast Augmentation using fat transfer focuses on improving breast appearance for patients who desire enlargement of their breast but who may wish to have an alternative to a silicone implant and for patients who may have failed implant augmentation. Patients are counseled regarding potential limitations of fat graft transfer to the breast when breast skin laxity is limited; this means that the breast skin may only accommodate a certain volume of fat graft that may be less than the desired volume of augmentation.
In such patients, the second session of fat grafting is recommended with a delay of at least six months between grafting sessions.
Breast reconstruction patients have greatly benefited from fat grafting advances because prior to its availability, patients had to compromise with their breast mound results. Several breast mound concerns can be corrected using fat transfer/grafting transplantation including:
- Visible breast skin wrinkles, termed rippling, are most visible along the medial breast pole as well as the inferior lateral breast pole.
- Residual breast mound size asymmetry is between implant sizes; this is because depending on the implant style selected, implant sizes are available in 50cc increments; this means that if you have a difference in size less than 50cc, you can utilize fat transfer to correct that volume difference.
- Upper chest contour concavity may be present when the mastectomy specimen extends up to the upper chest and axillary region that cannot be corrected with an implant only.
Buttock Augmentation, coined Brazilian Butt Lift, describes the transfer of fat which can be used to both augment the size of the buttock but also to reshape the butt and in revision cases correct contour irregularities. A recent advancement has involved the correction of cellulite, which are contour irregularities observed in the buttock cheek. This particular corrective surgery utilizes a novel 3 step process that involves:
- Redistribution of fat from areas of fat herniation to areas of concavity
- Release of oblique tethering ligaments
- Tightening of loosened fibro-septal network
Fat-grafting body dedicated to buttock enhancement has been the fastest growing sector in cosmetic surgery. Technical advances in multiple procedural steps have resulted in superior body contouring outcomes. Advances have included:
- Fat collection using VASER ultrasound energy. If you are interested in why VASER liposuction provides ideal Brazilian Butt Lift Results, please read the blog found on highdefinitionliposuction.com.
- Closed-loop system for fat collection and processing
- Closed-loop fat reinjection of fat into the buttock.
Fat Grafting Body Procedure
Improvement of facial wrinkles, folds, depressed cheeks, poorly defined jawlines, and lips; improvement of body contour irregularities following poorly performed liposuction; improvement in breast mound volume and shape in patients who have failed either breast augmentation with breast implant and patients who require revision of their breast mound shape following reconstructive surgery.
Fat Grafting Body Length
Ranges between 1 to 2 hours depending on the volume of fat transfer required.
Fat Grafting Body Anesthesia
General anesthesia or intravenous sedation depending on the volume of fat transfer required.
Fat Grafting Body Place of Treatment
Outpatient surgical suite or hospital operating room.
Fat Grafting Body Side Effects
- Prolonged swelling up to 2 to 3 weeks is not uncommon due to the overfilling of fat that is performed to compensate for an expected 30 to 40 % of fat graft loss that is observed over the first year following the fat transfer. Most patients will notice aesthetically pleasing results at 2 weeks following surgery and stable volumes of correction and filling at one month following surgery.
- Temporary bruising is often associated with fat transfer/grafting surgery due to the extent of tissue trauma that is created by fat harvesting and injection techniques. Bruising is minimized by compression dressings and ensuring that patients due not have any blood clotting disorders. Most bruising subsides within 1 to 2 weeks.
- Temporary numbness is not uncommon and secondary to inadvertent injury to small sensory nerves which are traumatized by the mechanical action of fat harvesting and injection cannulas. Fortunately, patients should expect a full return of sensation at These nerves even when traumatized will regenerate and re-establish sensation.
- Under correction void spaces, wrinkles, folds, contour deformities, or breast mound shapes is not uncommon as patients should expect 30 to 40% of volume loss that becomes apparent over the first year following surgery. Despite this expected volume loss, most patients are ecstatic with their postoperative observed volume corrections.
Fat Grafting Body Risks
- Deep vein thrombosis (DVT) may occur in the legs immediately following surgery requiring general anesthesia. DVT refers to the clotting off of leg veins which may result in compromised blood flow return from the legs; a more critical consequence may develop from this clot if it is dislodged and travels to the lungs causing pulmonary emboli. Although rare, pulmonary emboli are the leading cause of death following surgery. Measures are taken intraoperatively to avoid such a complication.
- Local skin or fat infection is uncommon and associated with individual patients with poor healing tendencies secondary to medical illnesses. Diabetes, nutritional deficiencies, and smoking are to blame for local infections. Well-controlled sugar levels in diabetic patients, optimizing nutrition, and cessation of smoking are critical to avoiding infections.
- Skin tissue compromise leading to skin loss is rare following fat grafting surgery and is associated with the filling of scarred tissues due to increased degree of undermining and tunneling required to transfer fat cells. Smokers are urged to stop smoking for 4 weeks prior to and for 6 weeks following surgery in order to minimize skin tissue compromise.
- Fat emboli syndrome is a rare risk factor that can be life-threatening if not detected in the early postoperatively. This
condition is caused by transferred fat cells entering major blood vessels and being dispursed and getting clogged in life-sustaining organs. Patients may present with a multitude of symptoms ranging from uncontrolled hypertension to chest pain, lightheadedness, confusion, and difficulty breathing. Patients require immediate admission to a hospital for supportive therapy with intravenous fluids and possible respiratory support until these fat cells self dissolve.
Fat Grafting Body Recovery
The recovery period for fat transfer/grafting surgery with a return to most daily activities ranges from 1 to 2 weeks. Patients are asked to forego physical activities and exercise for approximately 2 weeks following surgery. Finally, patients are asked to forego important social engagements for approximately 1 month until volumes of contour correction are stabilized.
Fat Grafting Body Duration of Results
Patients who have undergone fat grafting surgery can expect aesthetically pleasing results for life. Patients will observe 30 to 40% of volume loss over the first year following surgery. However, volume corrections one year following surgery should be considered stable.
FAT GRAFTING BODY FREQUENTLY ASKED QUESTIONS:
The first reported fat transfer was reported as early as 1893 by a German physician, named Franz Neuber, who injected fat to improve a facial pit caused by tuberculosis complications. Just 2 years later, another German physician, named Czerny transferred fat to the breast. This surgery was also considered the first documented breast augmentation in the world. For nearly a century fat transfer never gained popularity due to poor survivability following transplantation. For the last two decades, largely due to the efforts of a U.S. surgeon, Dr. Sidney Coleman, fat transfer has come back into vogue.
Good candidates for fat transfer/grafting procedure are patients who require filling of void spaces, wrinkles, folds, contour deficits, etc. These theoretical considerations result in a number of indications for surgical fat grafting. Recently, it has been recognized that patients who demonstrate facial aging signs such as drooping and sagging of tissues also demonstrate loss of volume. This loss of volume has been attributed to deflation of the fat underlying the skin. Several areas can now be successfully filled by fat grafting including the cheeks, jawline, laugh lines extending from the corner of the lip (those extending up are called nasolabial folds; those extending downward are called marionette lines), in the hollow of the lower eyelids, temple region, under the eyebrows, under the upper eyelid(if fat was over-resection following upper eyelid surgery), and the lips. Patients who have previously undergone liposuction by injection techniques or SMART lipo often present with contour deformities such as pitting, etc. These areas may be filled with fat grafting. Finally, patients who have failed breast augmentation with implants or breast reconstruction patients with residual contour deformities may benefit from breast mound filling or revision by fat grafting.
Fat grafting involves transferring of fat from areas with generous fat supply to areas lacking in fat content or areas requiring filling such as void spaces, wrinkles, folds, and contour deficits. Fat must be harvested using modified liposuction techniques which are meant to preserve fat cells. These modifications include lowering the pressure of the suction to less than 15mm Hg pressure instead of 25 to 30 mm Hg pressure used routinely during liposuction. In addition, the fat cells are handled gently while removing the excess fluid(plasma) from the fat. Finally, the fat cells are washed with 1 L lactated ringers fluid mixed with 80mg of Gentamycin. These fat cells must be harvested, processed, and transferred expediently in order to minimize outside exposure period. Fat cells are then loaded into syringes and injected into the tissue in order to sculpt and correct above discussed deformities. In order to ensure re-establishment of transplanted fat cell vascular supply, fat cells are transplanted in 0.1 to 0.2ml micropackets. Transplanting fat cells in micropackets maximizes surface area to volume thus optimizing re-establishment of vascular supply. Areas that are grafted will be gently and smoothly wrapped in order to maintain fat cells in their transferred location. Liposuctioned areas are also dressed with compression garments to ensure a smooth contour.
On your initial visit, your surgeon will evaluate your health status by obtaining blood work. If you are 50 years or older you will need to have an EKG of your heart to rule out any heart conditions. If you are a smoker, you should quit for 1 month prior to and six weeks following your fat grafting surgery to maximize your rate of fat graft take. The limitation of fat transfer/grafting surgery is the rate of fat graft take which is dictated by the rate at which transplanted fat cells regain their vascularity and thus preserve their viability. Since the fat cells are avulsed from their home and transplanted to a new environment, they must establish their vascular blood supply in order to survive. This effectiveness of fat cells to re-establish this vascular supply determines the success of fat grafting take and over all success. Nicotine adversely effects the small vessels of the skin and is detrimental to re-establishing the blood supply to fat cells. Finally, you will need to arrange for a friend if you don’t have a spouse to care for any small children who may need to be lifted or carried for the first few days following surgery.
Patients who undergo fat grafting surgery are extremely satisfied with their surgery and their more youth appearing faces, improved body contour, or more robust breast mound shape. By providing a thorough preoperative workup, a safe intraoperative course, and frequent postoperative visits, patients should expect a speedy recovery and effective postoperative results.
Since fat grafting surgery will require general anesthesia or intravenous sedation, it must be performed in an operating room that is part of a hospital institution or outpatient surgery center. Less frequently, patients may be operated on in an in-house office based operating room, but it is of utmost importance for patients to make sure that the office facility is accredited by a surgical accreditation body such as AAAASF.
For large facial fat transfer/grafting or breast augmentation or breast reconstruction revision general anesthesia is required. For correction of small contour deformities intravenous sedation may be utilized.
Patients will awaken from general anesthesia or intravenous sedation to find their fat grafting harvest sites covered by a compression dressing. The compression dressing ensures that areas which were liposuctioned turn our smooth in contour. When transferring fat to the body and/or breast areas, grafted areas will be wrapped with smooth compression dressings to ensure a smooth contour and to ensure that fat cells don’t migrate from their transplanted positions. When fat is transplanted to the face and lips, patients are asked to avoid unnecessary compression especially at nights by sleeping upright with several pillows to cushion each side of the face. Swelling and bruising is typical over grafted sites as over-correction and filling is recommended as up to 30 to 40 % of grafted fat volume is lost over one year period. Patients will notice resolution of swelling over one to two weeks. Arnica gel is recommended for patients demonstrating increased bruising postoperatively. Patients are asked to avoid strenuous physical activity for the first two weeks in order to avoid inadvertent bleeding. Patients can expect full recovery and satisfactory aesthetically pleasing results one month following surgery. Patients ma plan important social engagements as early as 4 weeks following surgery.
Patients can expect to return to work at 1 to 2 weeks following surgery if they work in the back office and do not have to be fully presentable. For patients who deal with consumers or are in sales, 2 to 3 weeks off of work may be more prudent. Finally, if patients have physically strenuous jobs, then two weeks of down time is recommended prior to return to work.
There are several side effects that have been associated with fat grafting surgery and included:
a) Prolonged swelling up to 2 to 3 weeks is not uncommon due to over filling of fat that is performed to compensate for an expected 30 to 40 % of fat graft loss that is observed over the first year following fat transfer. Most patients will notice aesthetically pleasing results at 2 weeks following surgery and stable volumes of correction and filling at one month following surgery.
b) Temporary bruising is often associated with fat grafting surgery due to the extent of tissue trauma that is created by fat harvesting and injection techniques. Bruising is minimized by compression dressings and ensuring that patients due not have any blood clotting disorders. Most bruising subsides within 1 to 2 weeks.
c) Temporary numbness is not uncommon and secondary to inadvertent injury to small sensory nerves which are traumatize by the mechanical action of fat harvesting and injection cannulas. Fortunately, patients should expect a full return of sensation as these nerves even when traumatized will regenerate and re-establish sensation.
d) Under correction void spaces, wrinkles, folds, contour deformities, or breast mound shapes is not uncommon as patients should expect 30 to 40% of volume loss that becomes apparent over the first year following surgery. Despite this expected volume loss, most patients are ecstatic with their postoperative observed volume corrections.
a) Deep vein thrombosis (DVT) may occur in the legs immediately following surgery requiring general anesthesia. DVT refers to the clotting off of leg veins which may result in compromised blood flow return from the legs; a more critical consequence may develop from this clot if it is dislodged and travels to the lungs causing a pulmonary emboli. Although rare, pulmonary emboli are the leading cause of death following surgery. Measures are taken intraoperatively to avoid such a complication.
b) Local skin or fat infection is uncommon and associated with individual patients with poor healing tendencies secondary to medical illnesses. Diabetes, nutritional deficiencies, and smoking are to blame for local infections. Well controlled sugar levels in diabetic patients, optimizing nutrition, and cessation of smoking are critical to avoiding infections.
c) Skin tissue compromise leading to skin loss is rare following fat grafting surgery and is associated with filling of scarred tissues due to increased degree of undermining and tunneling required to transfer fat cells. Smokers are urged to stop smoking for 4 weeks prior to and for 6 weeks following surgery in order to minimize skin tissue compromise.
d) Fat emboli syndrome is a rare risk factor that can be life threatening if not detected in the early postoperatively. This condition is caused by transferred fat cells entering major blood vessels and being dispursed and getting clogged in life sustaining organs. Patients may present with a multitude of symptoms ranging from uncontrolled hypertension, to chest pain, lightheadedness, confusion, and difficulty breathing. Patients require immediate admission to a hospital for supportive therapy with intravenous fluids and possible respiratory support until these fat cells self dissolve.
FAT GRAFTING BODY PATIENT-SPECIFIC QUESTIONS:
In order to be a good candidate for breast augmentation surgery, you must have enough fat depots on your body to allow for harvesting of fat in order to inject into the breast. Unfortunately, most small breasted patients are also quite thin and don’t posses enough fat to allow for a substantial volume of fat to be transferred. Remember, that overfilling by approximately 300 cc is required to compensate for the 30% of volume lost at one year following surgery. Thus, if you were considering 400 cc breast implants, you would want to be injected with approximately 700 cc of fat per breast. This requires liposuctioning approximately 1500 to 2000 cc of fat from your body as this will yield approximately 700cc’s of fat following processing. If you are fortunate to have a large depot of fat and small breasts, then you are a good candidate. In contrast, patients who have failed breast augmentation with breast implants are ideal candidates, as they have no other option for breast augmentation. In addition, they usually have stretched out their breast skin envelop prior to having the implants removed for infection, capsular contracture, etc. and so will have increased room to accommodate the fat injections. For patients who have a tight skin envelope, two separate sessions may be required to attain the desired breast volume.
Several areas can now be successfully filled by fat transfer/grafting including the cheeks, jawline, laugh lines extending from the corner of the lip (those extending up are called nasolabial folds; those extending downward are called marionette lines), in the hollow of the lower eyelids, temple region, under the eyebrows, under the upper eyelid(if fat was over-resection following upper eyelid surgery), and the lips. Volumes of injection include:
| Facial Region (each side) | Volume of injection (cc’s) |
| Upper lips | 1 to 2 |
| Lower lips | 1 to 2 |
| Nasolabial fold | 2 to 3 |
| Marrionette folds | 1 to 2 |
| Cheeks | 2 to 6 |
| Lower Eyelid hollow | 2 to 4 |
| Upper Eyelid hollow | 1 to 2 |
| Eyebrows | 1 to 3 |
| Temples | 2 to 4 |
| Jawline | 2 to 5 |
Fat grafting requires avulsion of fat cells from their residence where they maintain a vascular supply to a new environment where they possess no direct vascular supply. As a result fat cells are required to keep alive by obtaining their nutrients by virtue of diffusion until a direct vascular supply sprouts into them. During this delay prior to vascular supply reintroduction it is believed that approximately 30% of cells do not make it and are eventually reabsorbed by the body over a one year period. In order to optimize fat cell viability, fat cells are transferred in 0.1 to 0.2 ml micropackets so that their surface area to volume ratios are maximized. This allows more of the cells to live by diffusion until the vascular supply is re-established.
Cellulite or dimpling is a complication of liposuction and is most commonly observed following more recent liposuction techniques involving mesotherapy (injection of fat dissolving material) and/or SMART liposuction (laser liposuction). Due to uneven liposuction techniques and/or liposuction in areas that are considered contraindications patients may observe divots and cellulite formation. Areas that are considered liposuction contraindications include the back of the thigh, the area located between the flanks and the hips, the ankles, the calves, and the middle of the medial thigh. These areas have strong fibrous attachments from the skin to the underlying muscles and thus removal of fat from these areas only promotes tethering of the skin down to the pulley effect of these attachments tightening down. To correct these deformities, the patient’s divots will have to be grafted with fat to resist the cable effect of the fibrous attachments. In addition, patients may benefit from addition of fat to areas that have been over aggressively liposuctioned resulting in correction of contour deformities, i.e. divots.
Fat grafting requires modified liposuctioning of fat cells followed by processing of the fat cells, and finally re-injection of fat cells into void/deficient contour areas. Both harvesting of fat and injection of fat utilize micro-cannulas which are smaller version of cannulas used in liposuction. As a result postoperative pain associated with fat transfer/grafting is similar to liposuction procedures. Patients should expect to be sore for approximately one week. Patients often describe a dull muscle like soreness that you might experience after weightlifting.
HOW OUR PATIENTS FEEL ABOUT US:
